Perianal Fistulising Crohn’s Disease – Associated anorectal and fistula cancers: Systematic Review and Expert Consensus
Serre-Yu Wong 1, Cathy Rowan 2, Elvira Diaz Brockmans 3, Cindy C Y Law 4, Elisabeth Giselbrecht 4, Celina Ang 5, Sergey Khaitov 6, David Sachar 4, Alexandros D Polydorides 7, Leon Shin-Han Winata 8, Bram Verstockt 9, Antonino Spinelli 10, David T Rubin 11, Parakkal Deepak 12, Dermot P B McGovern 13, Benjamin D McDonald 11, Phillip Lung 14, Lilli Lundby 15, Amy L Lightner 16, Stefan D Holubar 17, Luke Hanna 18, Carla Hamarth 19, Jeroen Geldof 20, Anders Dige 21, Benjamin L Cohen 22, Michele Carvello 10, Cristiana Bonifacio 23, Gabriele Bislenghi 24, Corina Behrenbruch 25, David H Ballard 26, Emre Altinmakas 27, Shaji Sebastian 28, Phil Tozer 29, Ailsa Hart 18, Jean-Frederic Colombel 4
Affiliations Expand
PMID: 38871152
Free article

Abstract
A global TOpClass review and expert consensus outlining the small but significant risk of anorectal and fistula-associated cancers in long-standing perianal Crohn’s disease, with practical guidance on risk awareness and prompt investigation of new or changing perianal symptoms.
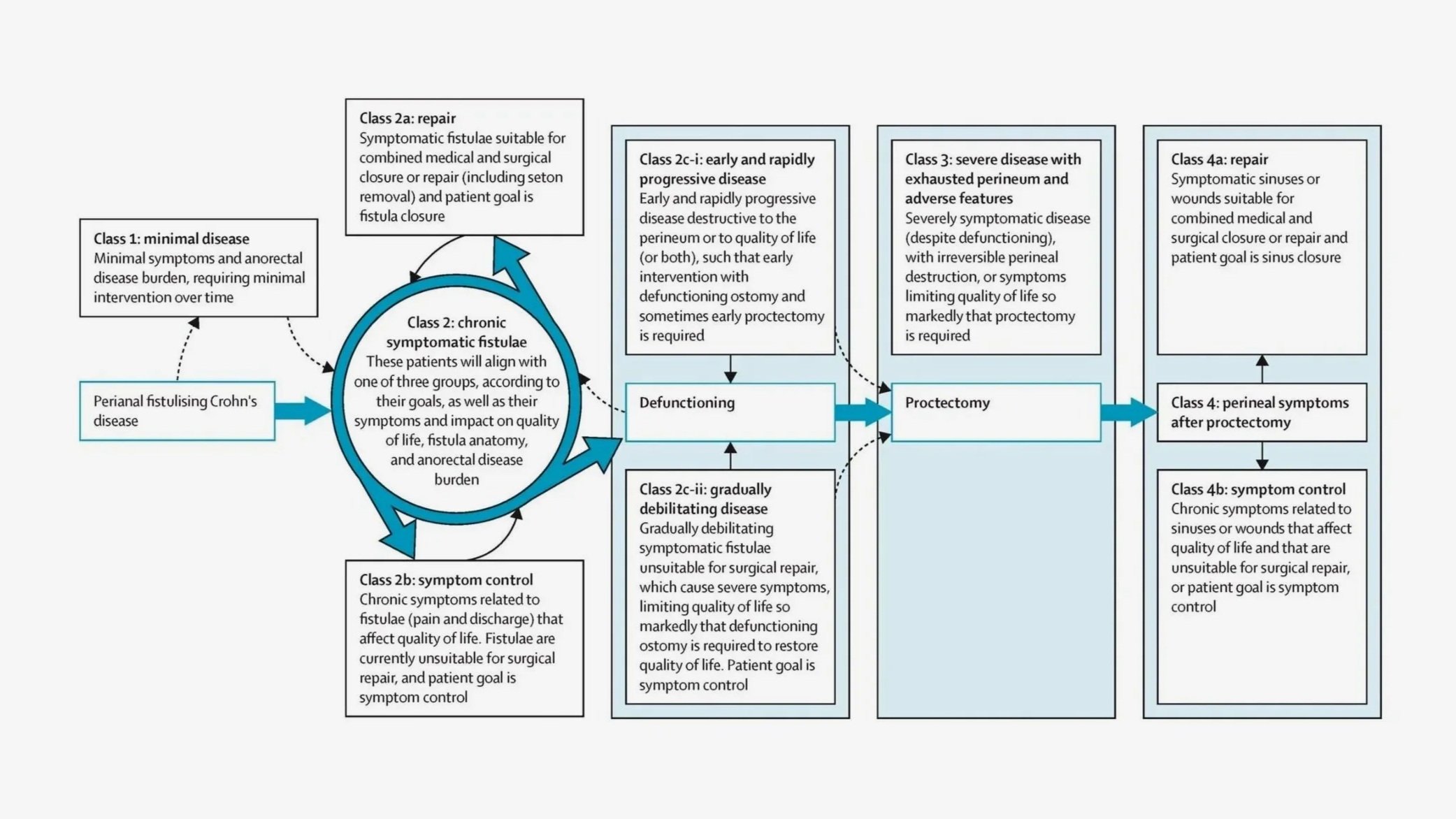
Background & aims: Perianal fistulizing Crohn's disease (PFCD)-associated anorectal and fistula cancers are rare but often devastating diagnoses. However, given the low incidence and consequent lack of data and clinical trials in the field, there is little to no guidance on screening and management of these cancers. To inform clinical practice, we developed consensus guidelines on PFCD-associated anorectal and fistula cancers by multidisciplinary experts from the international TOpClass consortium.
Methods: We conducted a systematic review by standard methodology, using the Newcastle-Ottawa Scale quality assessment tool. We subsequently developed consensus statements using a Delphi consensus approach.
Results: Of 561 articles identified, 110 were eligible, and 76 articles were included. The overall quality of evidence was low. The TOpClass consortium reached consensus on 6 structured statements addressing screening, risk assessment, and management of PFCD-associated anorectal and fistula cancers. Patients with long-standing (>10 years) PFCD should be considered at small but increased risk of developing perianal cancer, including squamous cell carcinoma of the anus and anorectal carcinoma. Risk factors for squamous cell carcinoma of the anus, notably human papilloma virus, should be considered. New, refractory, or progressive perianal symptoms should prompt evaluation for fistula cancer. There was no consensus on timing or frequency of screening in patients with asymptomatic perianal fistula. Multiple modalities may be required for diagnosis, including an examination under anesthesia with biopsy. Multidisciplinary team efforts were deemed central to the management of fistula cancers.
Conclusions: Inflammatory bowel disease clinicians should be aware of the risk of PFCD-associated anorectal and fistula cancers in all patients with PFCD. The TOpClass consortium consensus statements outlined herein offer guidance in managing this challenging scenario.
Related Research Groups














Browse Projects